Hysteria is a condition of psychic disturbance appearing in persons of nervous instability, when subjected considerable emotional strain or physical injuries.
CAUSES OF HYSTERIA
The exact cause is unknown.
Most probable causes are- Mostly female young and aged.
Heredity- family history is often present.
Characteristic hysteric type of personality is usually present.
Mental stress.
Constitutional factors.
SYMPTOMS OF HYSTERIA
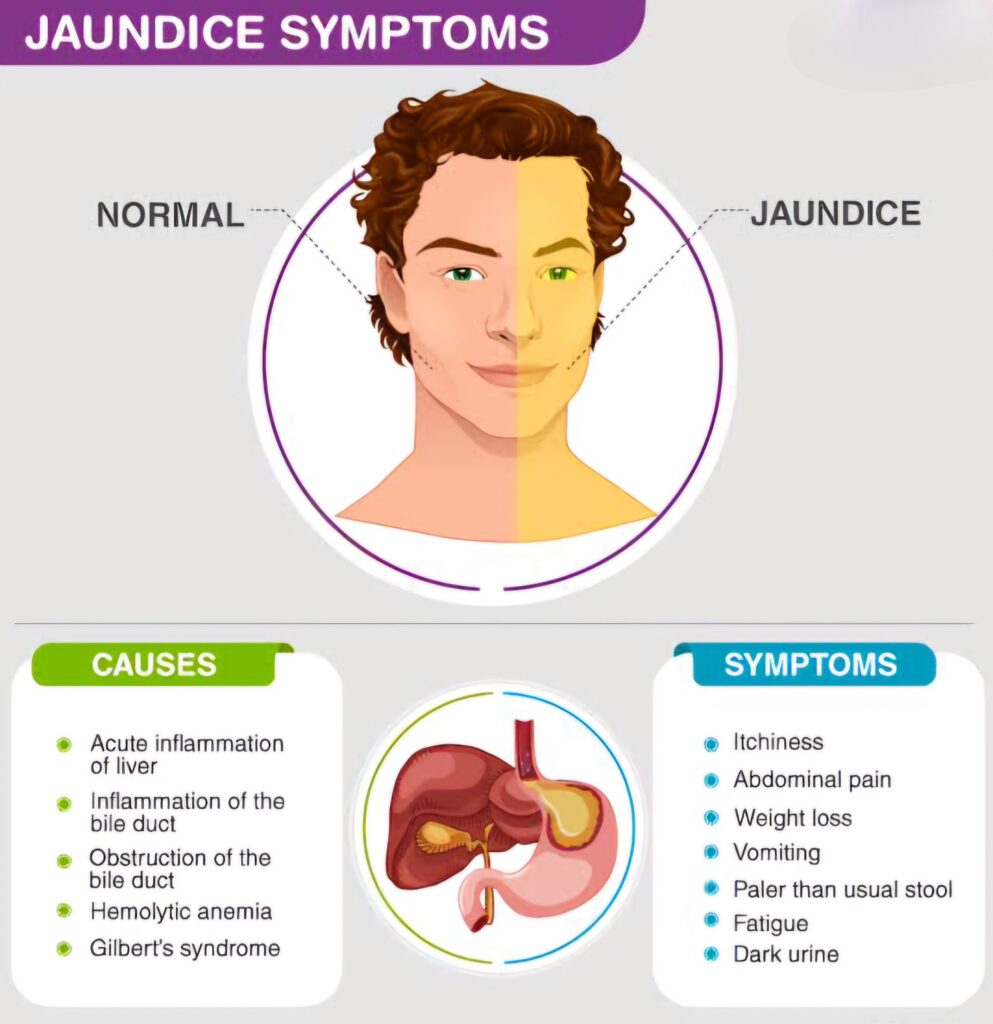
Sensory symptom- Blindness or deafness,anaesthesia and pain,deficiency of taste or smell hysterical abdominal pain, vomiting, may be present.
Motor symptoms – Paralysis, spasms and tremor. Hysterical fits occur when there is an audience and consist of a thrashing about the limbs with the eyesfirmly shut.
Mental symptoms – Loss of memory, delirious, hystericalpseudo-dementia, stupor, hysterical excitements, hysterical phobias, hystericalanxiety & depressive states. There may be ceaseless laughing or crying.
Other symptoms – Compensation neurosis, engagement neurosis, anorexia nervosa, breathlessness, palpitation, praecordial pain, blepharospasm, mutism,aphonia, explosive utterances or stammering may be present.
The characteristic points are – wasting, loss of response to electrica lstimuli and aberration of tendon or superficial reflexes or of sphincter control asare found in organic nerve lesions, absent.
PROGNOSIS
It depends on the personality, environment andtreatment adopted.
MANAGEMENT
The treatment of hysteria is mainly psychological.
Relief of focal symptoms may be given by suggestion, persuasion or by re-education.Underlying cause should also be treated. Supportive, interpretative or other methods of psychotherapy may be employed. Environmental factors should be readjusted as far as possible. Gradually- patient is to rehabilitate intonormal activities.
Drug treatment – this has probably no role except when depression or anxiety neurosis plays some part in the background (for mental satisfaction of the patient, placebo may be prescribed.
Angina Pectoris is ,Ischaemic cardiac Pain of short duration due to lack of sufficient amount of oxygenated blood supply to the cardiac musculáture. (Or, it is a form of ischaemic heart disease; marked by paroxysmal attacks of substernal pain without evidence of lasting damage to the myocardium).
CAUSES OF ANGINA PECTORIS
Exact cause or aetiology is unknown. Predisposing factors:
Age: middle age.
Sex: male predominate.
Habit – Smoking.
Food habit – Fatty and hypertensioned personsare more affected.
Vascular resistance Anoxaemia (a) anaemia; (b) high altitude ncreased work of the heart – (a) hypertension; (b) valvular disease.
Precipitating causes -(a) muscular exercise; (b) exposure to cold;(c) heavy meal, etc.
Psychogenic factor – mental anxiety.
SYMPTOMS OF ANGINA PECTORIS
Angina Is essentially a type of pain thus itself a Symptom.
Pain in chest.
Location -Mid or upper sternal region; may be felt over the left side of chest.
Nature of pain – Classically constricting,_squeczing pressing, or crushing in character, sometime numbing or burning.
Duration – usually not more than 2 – 5 minutes. Any cardiac pain of more than 5 min is never due to angina pectoris.
Provoking factors usually starts by walking up hill or against the wind, after exertion.weight lifting, emotion, by_ hurrying after meals or heavy meal, by exposure-to cold or by unaccustomed exercise.
Pain may_also- be induced by excitement,_anger, fear or apprehension, even during sexualintercourse.
Relief – Usually disappears after taking rest for a while or after taking nitroglycerin.
SIGNS
Classical signs are present only during attack. T (a) Decubitus – propped up. (b) Attitude – Closed fist kept over the chest. (c) Face – Deathly pale and anxious. (d) Pulse – Increase. (e) Respiration – Hurried and shallow. (f) Blood Pressure – may or may not be raised. (g) Shortly after an attack, tender spots may be present over the praecordium or along the arms. (Cardiac finding- usually nil. Heart block
Systemic signs – During attack. . Auscultation = Tick-tack rhythm, S4 and S5 may be audible (gallop rhythm), apex beat may be shified downwards.
E.C.G. (may or may not show per ischaemic changes ordinarily) STSegment depression flattening of T wave or sometime elevation of`STsegment.
Selective coronary angiography – In many cases it mayshow definite narrowing of coronary artery in more than two segments.
TYPES OF ANGINA PECTORIS
Stable angina This is classical angina pectoris shown due to exercise.
Unstable angina Same over it is severe; pain occurs in night, duration of pain 15 minutes or more.
Variant angina Periodical waking and waning to time fixation.
PROGNOSIS
Prognosis is worse in the patient who has had multiple cardiac infarcts or who has cardiac failure or who has a family history orcoronary disease. Many men have continued to live for many years by restricting their activities & full expectation of life have been achieved.
MANAGEMENT
Patient should be instructed to lead restful life avoiding mental anxieties,worries, smoking and all other provoking factors.
Physical activities should be minimized.
In obese subjects adequate diet chart should be followed so as to reduce the body weight.
SOMETIMES SURGICAL PROCEDURES MAY BE DONE IN EMERGENCY CASES.
It means recurrent sudden attacks of unconsciousness caused by impaired conduction of the impulse that regulates the heartbeat; often applied specifically to atrioventricular heart block.
HEART BLOCK CAUSES
Depression of conductivity is most commonly due to ischaemia, fibrosis or inflammation of the A. V. bundle.or to vagal stimulation.
Myocardial infarction is the commonest cause.
Idiopathic focal fibrosis – is a common cause of chronic heart block.
Rheumatic fever and Diphtheria.
Drugs, e-g., Digitalis,quinine etc.
Cardiomyopathies.
Disordered.atrial rhythms, .e.g.auricular fibrillation and flutter.
Congenital causes, e.g. ventricular
septal defect or maldevelopment of the bundle, etc.
Aortic stenosis
TYPES OF HEART BLOCK
First Degree – All S.A, impulses are allowed to pass through A,V. node but the time is prolonged.
Second Degree – Here S.A. impulses are not allowed to pass through A. V. node from time to time.
Third Degree of complete heart block -Here no S. A. impulses are allowed to pass through A. V. node,therefore ventricles generate their own rhythm 30 to 40 per minute.
Whooping cough (or, Pertussis) is an acute infectious,communicable disease affecting the respiratory tract, characterized by spasmodic attacks of coughing & accompanied by an inspiratory whoop.
Season -usually colder months.. Spread -by droplet infection
PATHOLOGY‣ The whole respiratory tract from nasopharynx down to bronchi is involved in a narcotizing inflammation along with inflammation of the peri-bronchial and tracheobronchial lymphoid tissue. The stickiness of exudate is responsible for obstruction of bronchioles leading to atelectasis.
SYMPTOMS
Incubation period 01 to 03 weeks.
CLINICALs Catarrhal stage: Duration – one week withgradual onset.
Dry cough, vomiting occasionally following a severe bout of cough.
Anorexia and insomnia.
Sneezing, coryza and lacrymation (sometimes conjunctivitis).
Moderate fevers.
Paroxysmal Stage: Duration – 2 to 4 weeks.
Cough(paroxysmal) 30 to 50 times a day. thick mucoid sputum and vomiting maybccur at the end of bouts.
‘Glottis may have ulcer, spasm and oedema.
Tetany due to severe vomiting.
Bleeding tendency i.e. haemoptysis, epistaxis, purpura,Whoop immediately following the intestinal haemorrhage may occur.
Convalescent Stage: Usually begins within 4 weeks after the acute onset.
Cough becomes less frequent and sputum is less tenacious.
Vomiting may rarely occur as a matter of habit.
Improving appetite.
Immunity after illness lasts long.
INVESTIGATION
CBC
ESR
SPUTUM CULTURE
X-Ray Chest
PROGNOSIS
Better in older children and in the aged but comparatively worse below 03 years.
PROPHYLAXIS
Triple antigen should be given in a dose of 1-cc subcutaneously after every month for three doses. Booster doses after one year and once again before going to school.
COMPLICATIONS
Pneumonia
Emphysema
Dyspnea
Toxic Encephalitis
Pneumothorax
Umbilical hernia
Convulsions
Meningitis
Cerebral hemorrhage
Enteritis
Otitis media
Fulminant Tuberculosis
MANAGEMENT & TREATMENT
Bed rest in a well ventilated calm and quiet room during catarrhal stage and for a time during paroxysmal stage.
Diet liquids and semi solid diet, feeds should be given immediately after vomiting or paroxysms and should be small & frequent.
Cough suppressants may also be used, e.g. phensedyl (promethazinecodeine, ephedrine) .
Sedativeday Satriclofos (Tricloryl) syrup 250-mg.
Antibiotics tetracycline 50-mg- per kg of body weight daily in divided doses (or Ampicillin 150-mgm. per kg of body wenght.Erythromycin 50-mg. or Hyper-immune convalescent serum 20-ml. intravenously at 2-3 days intervals.
All treatment should be given on the instructions of your Physician.
It is an allergic condition characterised by paroxysmal attacks of dyspnoea accompanied by wheezing,chiefly expiratory in nature,associated with bronchial spasm.
TYPES
Extrinsic – Starts in childhood,becomes alright in adult life.
During the attacks,lungs are voluminous and emphysematous,filling the entire pleural cavities Area of emphysema alternates with the areas of atelectasis or collapse.If asthma associated with bronchitis,emphysema ensues.
SYMPTOMS
Dyspnea
Cyanosis,pale.
Tachycardia
Wheezing Sound during respiration.
Anxiety
Breathless
Chest pain
Severe Cough(Occurs at night)(dry or with phlegm)
INVESTIGATION
X-Ray Cest
CBC
ESR
Sputum Culture
Test By Spirometry
Peak flow test
Allergy Test
Sinus X-ray
COMPLICATIONS
Lung infection
Status Asthmaticus.
Bronchitis or Tuberculosis
Emphysema of lungs
Bronchiectasis
Heart Attack
PROGNOSIS
The individual attacks is good ,except in severe status asthmaticus where there is occasionally a fatal outcome.Spontaneous recovery is fairly common in episodic asthma,particularly in children,but rare in chronic asthma,which often causes permanent pulmonary damage.
PREVENTION
Prevention of cold ,dust,infection,food avoid allergens.Rest in bed in propped up position on a back rest or sitting up in a chair which one is comfortable.Control of infection by appropriate antibiotics.
MANAGEMENT & TREATMENT
Anti Inflammatory Drugs Should be use.
Psychotherapy make good role.
Bronchodilators Uses makes better relief.
Inhaler and Inhaled Corticosteroids.
Deriphyllin, Theophylline Ampicilin,Azithromycin.
Nebulization is first .(Asthalin ,Budecort)
In Chronic and Severe conditions O2 applied.
Breathing Exercise, Yoga And meditation.
Follow the prevention and instructions given by your Doctor.
Myocardial infarction commonly known as Heart Attack,it occurs when oxygen supply to heart muscles becomes nil, due to occlusion of one of the branches of coronary artery.
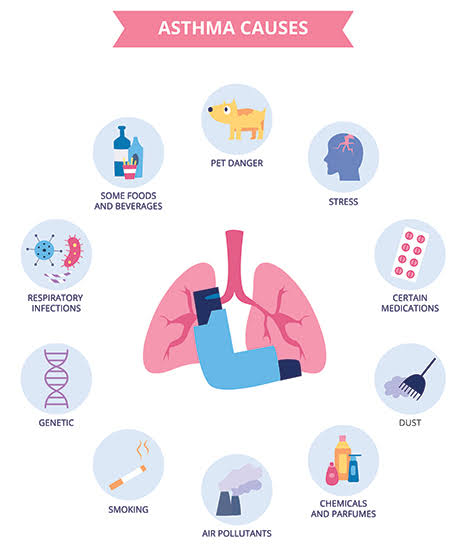
CAUSES–
Coronary Thrombosis
Coronary Embolism
Sub-intimal haemorrhage
Critical lowering of blood pressure
Syphilitic aortitis
RISK FACTORS
AGE- Commonly After 50 Years.
Sex- Mostly Men
Hypertension
Obesity
Stress
Smoking ,Alcohol,Unhealthy Diet.
Diabetes
Gout
Burger’s Disease
Polycythaemia
Hyperthyroidism
Brisk Haemorrhage as in – (A)- Peptic ulcer (B)- Surgical Operation
SYMPTOMS –
Breathlessness ,Restlessness
Cough,Sputum,Haemoptysis
Shock
Severe Sweating
Pain- Mild to Severe mostly in the middle of Chest with Left Shoulder and Arm. Jaw and Neck
In About a quarter of all cases of Myocardial Infarction death occurs within the first few minutes without medical care. If there will be no complications within the first four weeks,the Prognosis is favourable.
Sudden death under 40 is not uncommon.Unfavourable features are old age,cardiogenic shock,Cardiac failure,heart block and ventricular arrhythmias.
PREVENTION OF HEART ATTACK-
According to the World Health Organization, as many as 80% of all heart attacks and strokes are preventable. The majority of deaths due to CVD are precipitated by risk factors such as high blood pressure, high cholesterol, obesity, or diabetes, which can, to a large extent, be prevented or controlled through the consumption of a healthy diet, regular exercise and avoiding tobacco. Keeping an eye on your blood pressure, cholesterol levels and blood sugar levels is also very important.
Eat healthy
Stay Active
Lose or manage your weight
Get healthy sleep
Manage your blood pressure
Manage your Blood sugar level
Lower your cholesterol
Don’t Smoke
Avoid Alcohol
Manage your stress
MANAGEMENT & TREATMENT-
First Aid
If you think someone is having a heart attack:
If the person is unconscious and unresponsive, does not have a pulse, and an automated external defibrillator (AED) is immediately available – follow the instructions on the AED device.
Have the person sit down, rest, and try to keep calm.
Loosen any tight clothing.
Ask if the person takes any chest pain medicine, such as nitroglycerin for a known heart condition, and help them take it.
If the pain does not go away promptly with rest or within 3 minutes of taking nitroglycerin, call for emergency medical help.
If the person is unconscious and unresponsive, and not breathing or does not have a pulse, call the local emergency number, then begin CPR.
If an infant or child is unconscious and unresponsive, and not breathing or does not have a pulse, perform 1 minute of CPR, then call the local emergency number.
TREATMENT –
Types of medications
Heart attack treatment involves a variety of drugs. The following list provides an overview of the common types. You can also learn about medication in more detail.
Your health care team will recommend the best combination of medications for your situation.
Anticoagulant: Sometimes called blood thinners, these medicines make it harder for clots to form and also keep existing blood clots from getting larger.
Antiplatelet agent: Keeps blood clots from forming by preventing blood platelets from sticking together.
Angiotensin-converting enzyme (ACE) inhibitor: Relaxes blood vessels and allows them to expand while decreasing resistance by lowering levels of angiotensin II. Allows blood to flow more easily and makes the heart’s work easier or more efficient.
Angiotensin II receptor blocker: These medicines inhibit angiotensin II from having effects on the heart and blood vessels. This keeps blood pressure from rising.
Angiotensin receptor neprilysin inhibitor: Neprilysin is an enzyme that breaks down natural substances in the body that open narrowed arteries. By inhibiting neprilysin, those natural substances can have their normal effect. That improves artery opening and blood flow, reduces sodium (salt) retention and decreases strain on the heart.
Beta blocker: Makes the heart beat slower and with less force, which lowers blood pressure.
Combined alpha and beta blocker: Combined alpha and beta blockers may be used as an IV drip for people in hypertensive crisis. They may be prescribed for outpatient high blood pressure use if the person is at risk for heart failure.
Calcium channel blocker: Interrupts the movement of calcium into the cells of the heart and blood vessels. May decrease the heart’s pumping strength and relax the blood vessels.
Cholesterol-lowering medications: Various medications can lower blood cholesterol levels, but statins are the best first course of action. When statins don’t work, or if a person has serious side effects from statin therapy, other drugs may be recommended.
Vasodilator: Relaxes blood vessels and increases the supply of blood and oxygen to the heart while reducing its workload. Available as pills to be swallowed, chewable tablets and as a topical application (cream).
Common medical procedures following a heart attack
You’ll find many common medical procedures for heart attack listed here. For more detailed explanations of these treatments, see our page devoted to cardiac procedure.
Angioplasty: Special tubing with an attached deflated balloon is threaded up to the coronary arteries. The balloon is inflated to widen blocked areas where blood flow to the heart muscle has been reduced or cut off.
Laser angioplasty: Similar to angioplasty except the catheter has a laser tip that opens the blocked artery.
Heart valve surgery: Repairs an abnormal or diseased heart valve or replaces it with a healthy one.
Atherectomy: Similar to angioplasty except the catheter has a special tool on its tip to cut away plaque from the artery.
Bypass surgery: Treats blocked heart arteries by creating new pathways around the clot so blood can flow to your heart muscle.
Minimally invasive heart surgery: An alternative to standard bypass surgery using small incisions.
Stent procedure: A stent is a wire mesh tube that is placed during angioplasty to hold open an artery and restore blood flow.
Transmyocardial revascularization (TMR): A laser is used to drill a series of holes from the outside of the heart into the heart’s pumping chamber.
In addition to the above treatments, you might hear about implantable medical devices being used to treat certain conditions that increase risk of heart Attack.